
Tuberculosis contact investigation: A qualitative study to identify barriers, facilitators, and design opportunities in the improvement of identification of TB contact and key-patients and follow-up treatment
J. Jiménez-Garcia, J.E. Figueroa, G. Diaz, A.M. Victoria, Y. Niño-Ramírez, C.N. Rojas-Zúñiga, S. Melenge, V. Palacios, B.E. Ferro, J.L. Davis
Involvement: Principal Investigator
Partner: Universidad Icesi, CIDEIM, Alcaldía de Cali
Period: February 2019 – presentResearch project funded by Colciencias
Key words: qualitative study, generative research, design thinking, tuberculosis, participatory design.
Intervention
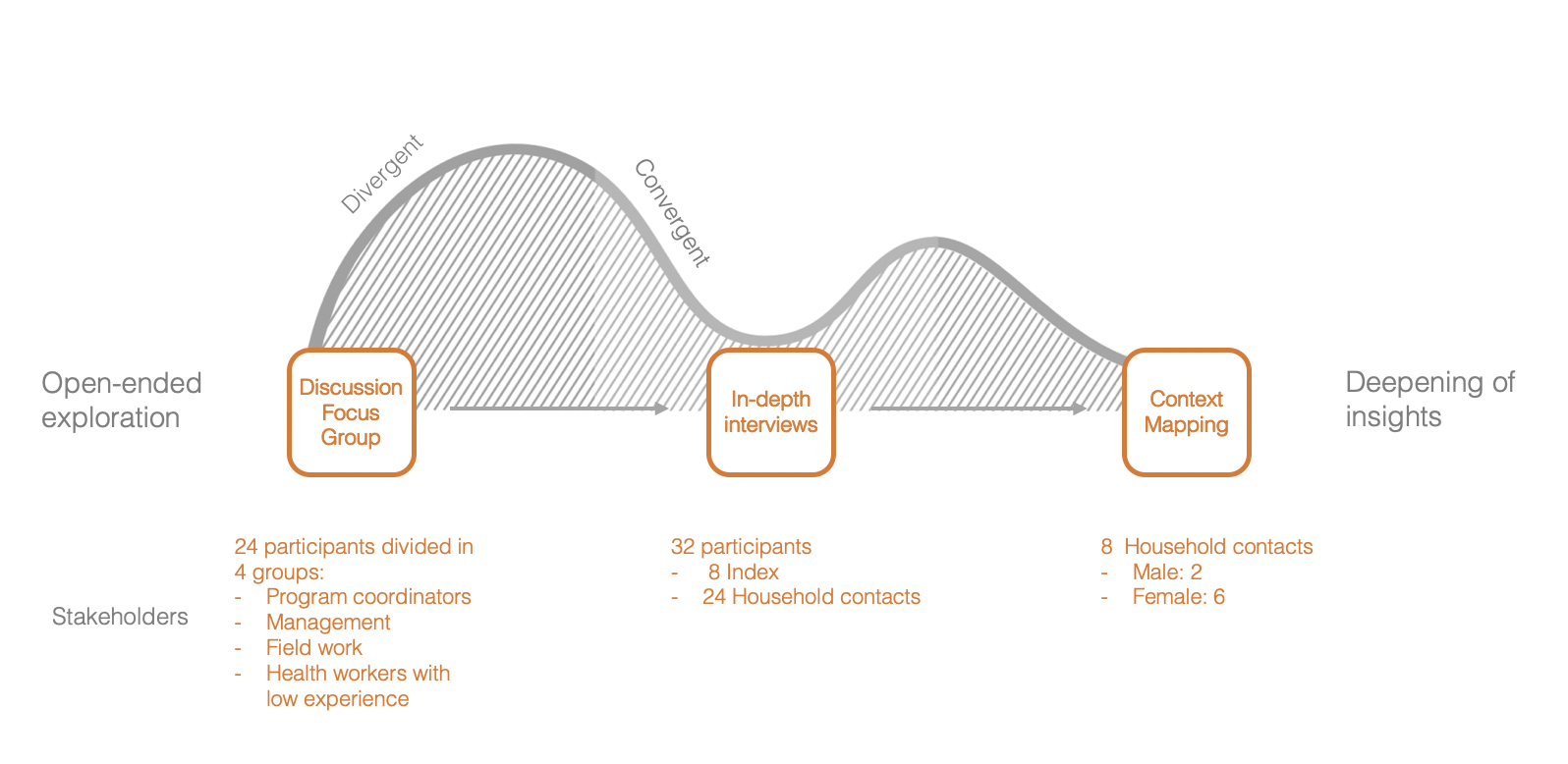
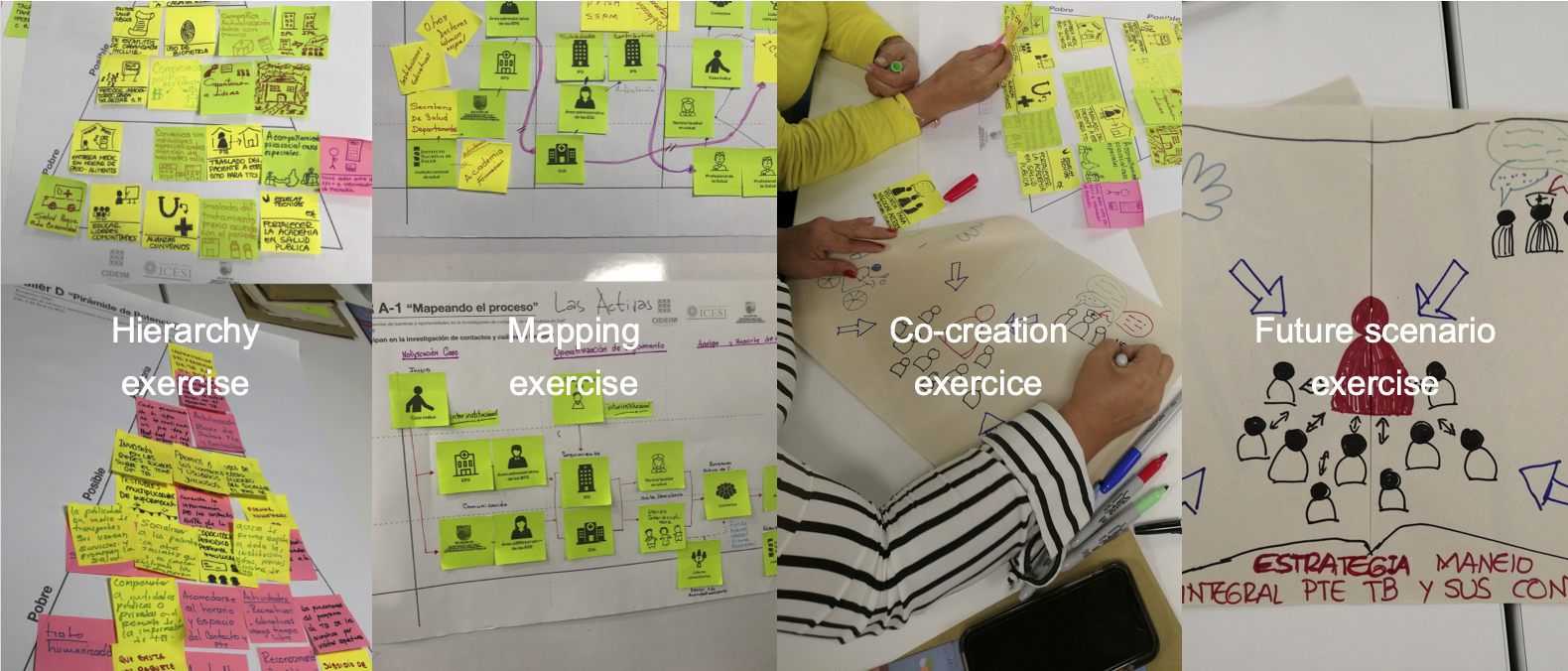
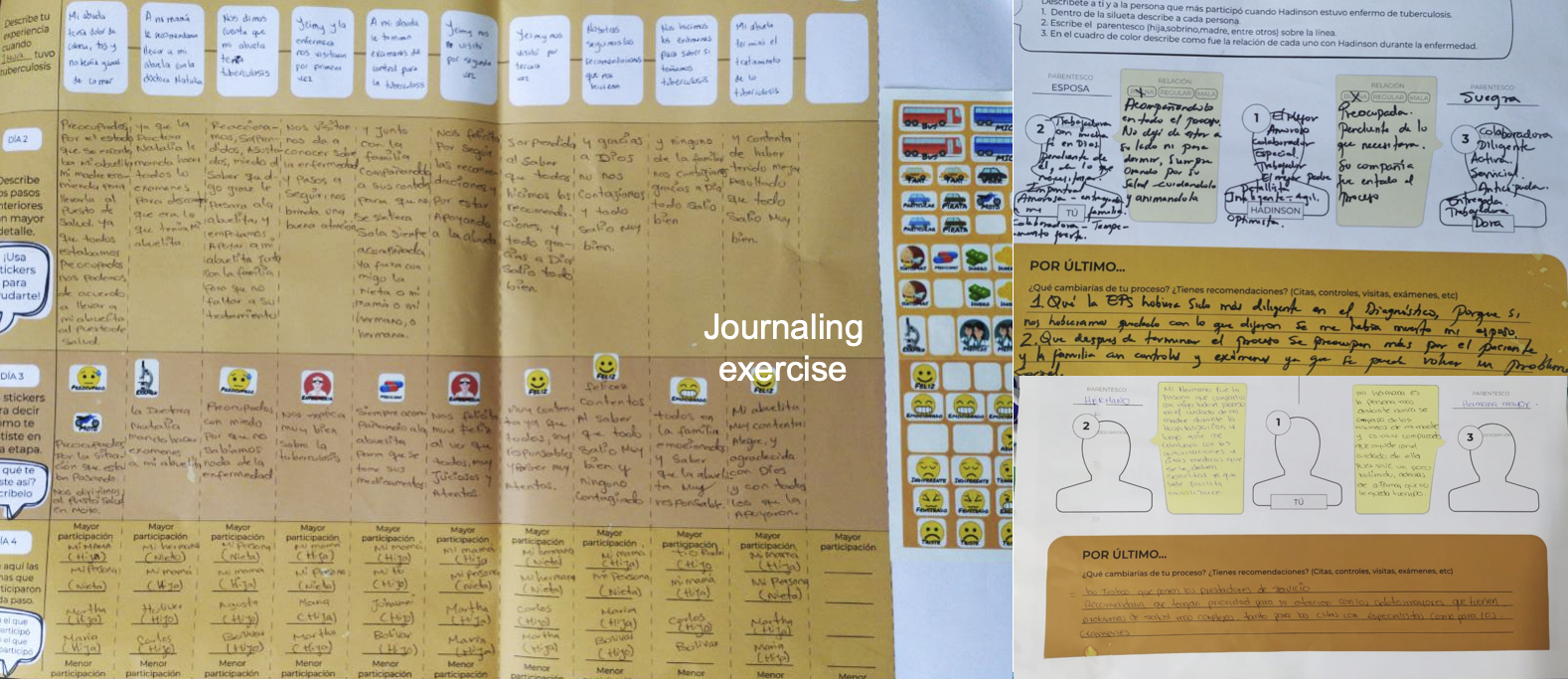
With a cross-sectional qualitative study combining human-centered design, social science methods, and a knowledge-growing strategy, we conducted three activities involving different stakeholders: a) focus-group discussion (1) with program coordinators and health-care workers, b) in-depth interviews with index TB patients (8) and household contacts (16), and c) context mapping sessions (6), with purposive selection of contacts. After consent, activities were audio-recorded and professionally transcribed. Using grounded theory, we generated and applied codes and categories to emergent themes until we achieved data saturation for each activity.
Results
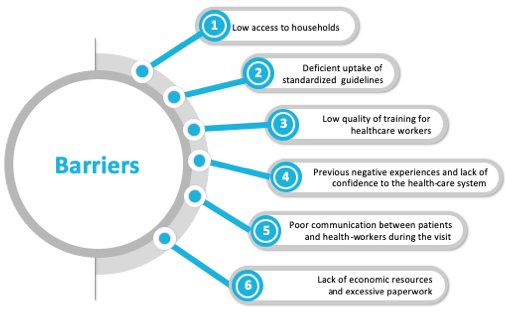
Common barriers are associated with low access to households (violence and lack of transportation into informal settlements, inaccurate data recording), deficient uptake of standardized guidelines, low quality of training for health-care workers; previous negative experiences and lack of confidence to the health-care system were perceived by patients and their contacts, poor communication between patients and health-workers during the visit, lack of economic resources and excessive paper-work were the final barriers for contacts’ evaluation. Significant facilitators included resourcefulness, empathy and delivery of clear information about TB from health-care workers; whilst family and social support and interest in remaining healthy was key for patients and contacts.


Conclusions
Household contact investigation in Cali could be improved by 1) enhancing personal skills and training of health-care workers with the use of standardized TB educational materials, 2) facilitating access to households by involving community leaders and implementing digital communication tools, and 3) defining a step by step attention route for patients and contacts, that involves a standardized data recollection system.

