

Designing reflective healthcare informatics: supporting patients during recovery at home.
PhD
Juan Jiménez Garcia.
Partner: Orthopaedic Department, Reinier de Graaf Gasthuis Hospital
Period: October 2009 – December 2014
Faculty of Industrial Design Engineering, TUDelft.
Research project funded by SENIOR consortium (Sensing Systems for Interactive Home-based Healthcare and Rehabilitation).
Key words: elderly, patients’ experience, experience sampling method, personal informatics, total hip replacement, healthcare.
The challenge
ESTHER, an Experience Sampling tool for Total Hip Replacement (THR) addresses the challenge to design tools that fit in the user’s home context and recovery process. ESTHER is an in-situ ecological design tool aims to capture an acute view of the life of THR patients during recovery at home. It samples and assesses two types of data: a) Objective (quantitative) data collected from sensors and b) subjective (qualitative) data collected from patients’ event of sequences in daily life and moods. The tool determined their needs regarding hip recovery and their variations over time by integrating these data and providing rich information to take informed actions. The value of this tool is to facilitate reflective mechanisms to support patients’ empowerment, with the potential to support physiotherapists and caregivers about the recovery process with the collected data.
The current healthcare paradigm shifts towards considering the patients’ home as the primary self-care environment. Homecare technologies can focus on supporting a reflective approach by providing users with relevant information that they can reflect upon, making them self-managers who are in control of their own care. In contrast, technologies that are only assisting the patient, commonly assume a more data-centric approach, in which the system takes a prominent role by nudging people towards a goal.
In order to design for supportive technologies that remotely support patients in their rehabilitation process and help users in identifying opportunities to change behavior, the major challenge ahead lies in designing technologies such that they become part of the users’ daily life activities.
The approach
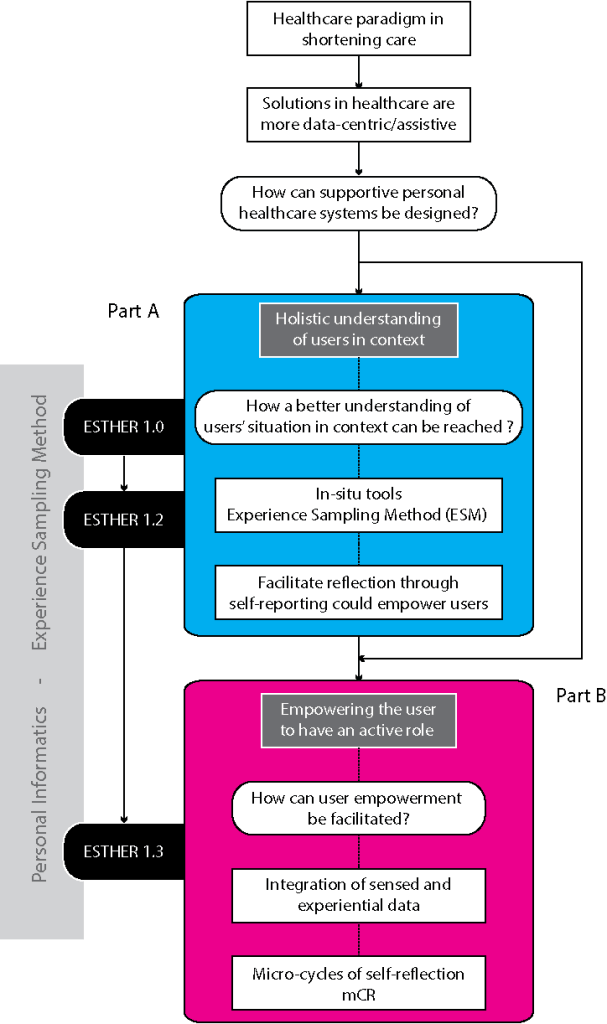
An integrated patient-centric approach was defined by zooming in from the general user context to a centralized focus on user experience. User-Centred Design Methods (UCD), Experience Sampling Method (ESM) and Personal Informatics (PI) framed a different stage of an iterative design and implementation of several prototypes. This approach differs from previous attempts to reach the user in that it assumes the challenges of considering users’ personal experiences and social context, collected in-situ, as crucial aspects when providing care support, which makes the research process more representative on real users’ daily life needs and desires
Three prototypes where tested in the field. ESTHER 1.0 studied the value to facilitate reflective mechanisms. In ESTHER 1.2, the in-situ self-reporting principle was extended with contingent experience sampling by means of on-body sensor nodes as it addressed the technical challenges of integrating self-reporting and automatically collected sensor data. ESTHER 1.3 was built to expand upon a design model for developing future personal reflective interfaces.
Design process
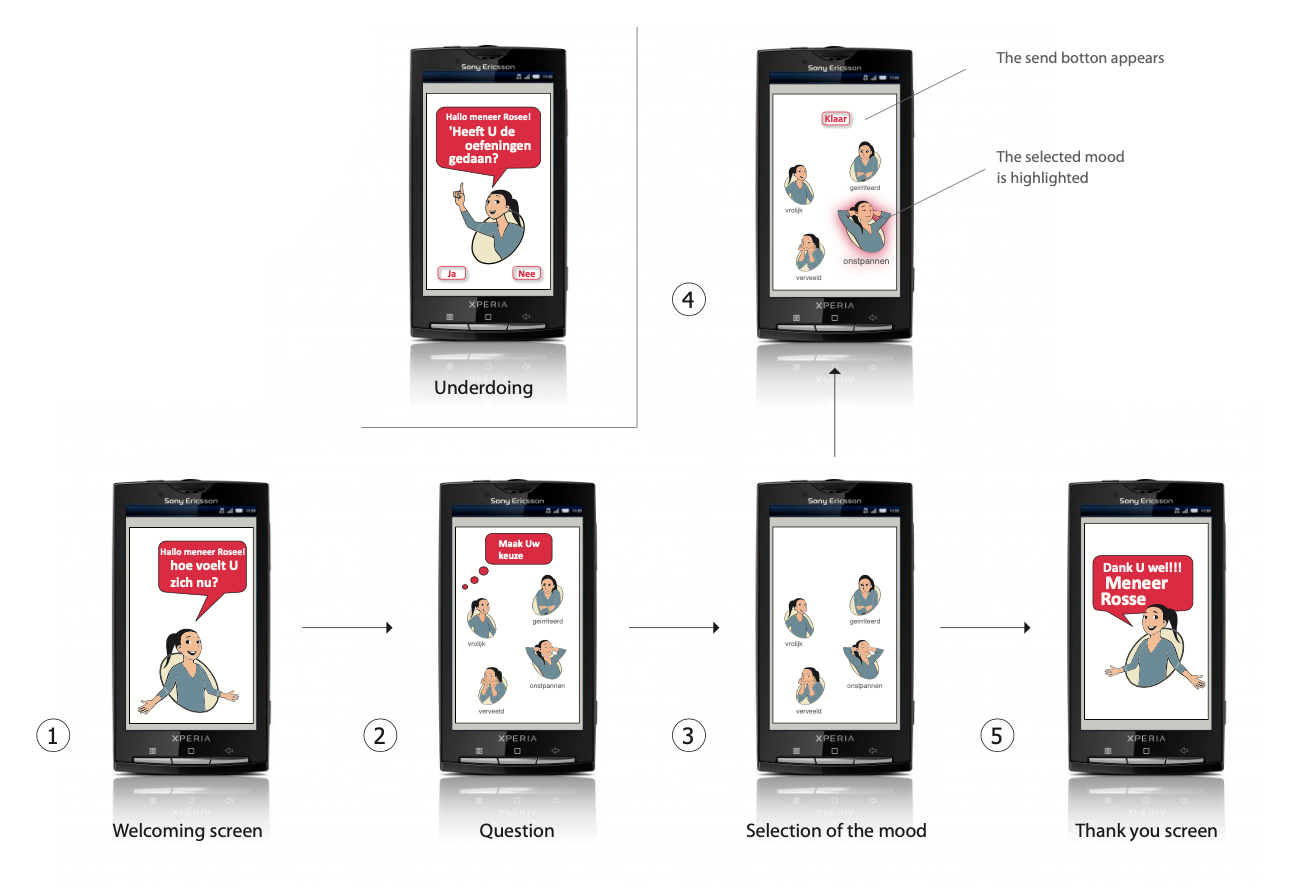
ESTHER 1.0 was designed as an in-situ, self-reporting tool that provides contextual and experiential variables by patients during their home recovery process. Based on Experience Sampling Method (Larson and Csikszentmihalyi, 1993), this tool provided a fixed interval sampling protocol using a step-by-step interactive questionnaire embedded in a tablet. The Pictorial Mood Reporting Instrument, PMRI, (Vastenburg et al., 2011) was chosen, as an easy-to-use mood capturing technique. The design of the tool was informed by focus groups observational testing sessions.


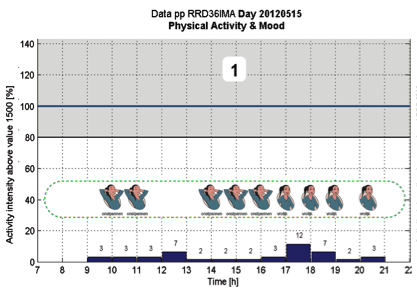
ESTHER 1.2 added to users’ psychological reports, physical activity using wireless sensor nodes. As conceived with ESTHER 1.0, a female character was used to host the tool, triggering the questions and guiding the patient through the application in a friendlier looking way. The tool was implemented on a mobile phone that was connected to a wearable sensor. The data coming from the sensor was used to identify ‘critical moments’ during THR recovery.


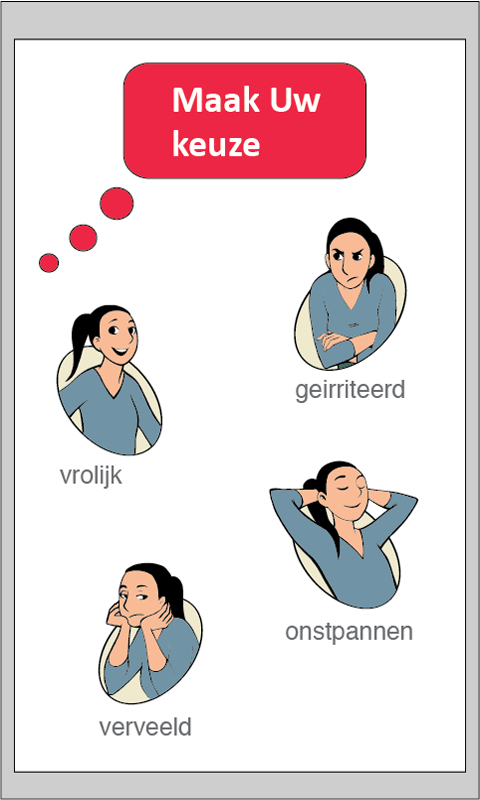
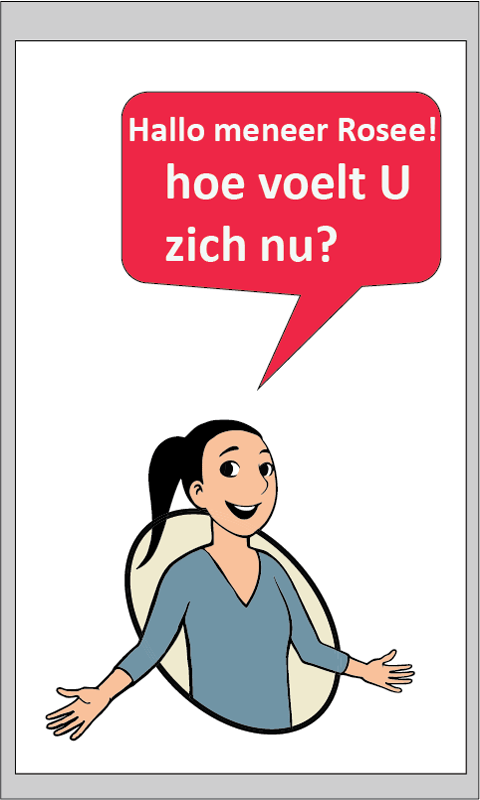
ESTHER 1.2. A female character was used to host the tool, triggering the questions and guiding the patient through the application in a friendlier looking way (based on the Pictorial Mood Reporting Instrument, PMRI.
Vastenburg et al., 2011)
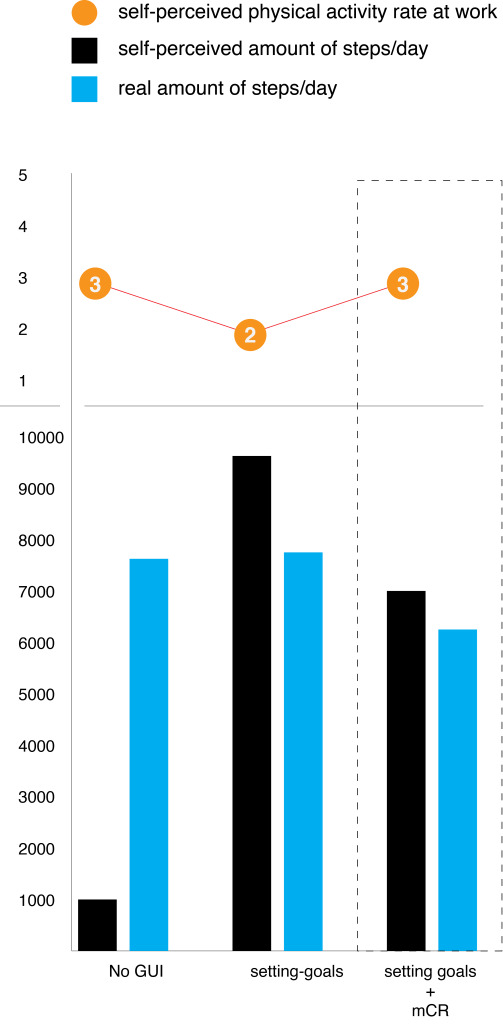
ESTHER 1.3 as subsequent design iteration, explored the value of self-reporting prompting as a reflective mechanism in a different scenario. It aims to support knowledge workers in the context of physical activity during working hours through self-reflection. This tool implemented the concept of “micro-Cycles of Reflection (mCR)” (Jimenez, 2015) to activate patients in the phases of integration and reflection when applying the staged-model of Personal Informatics (PI) (Li, 2010).

Results
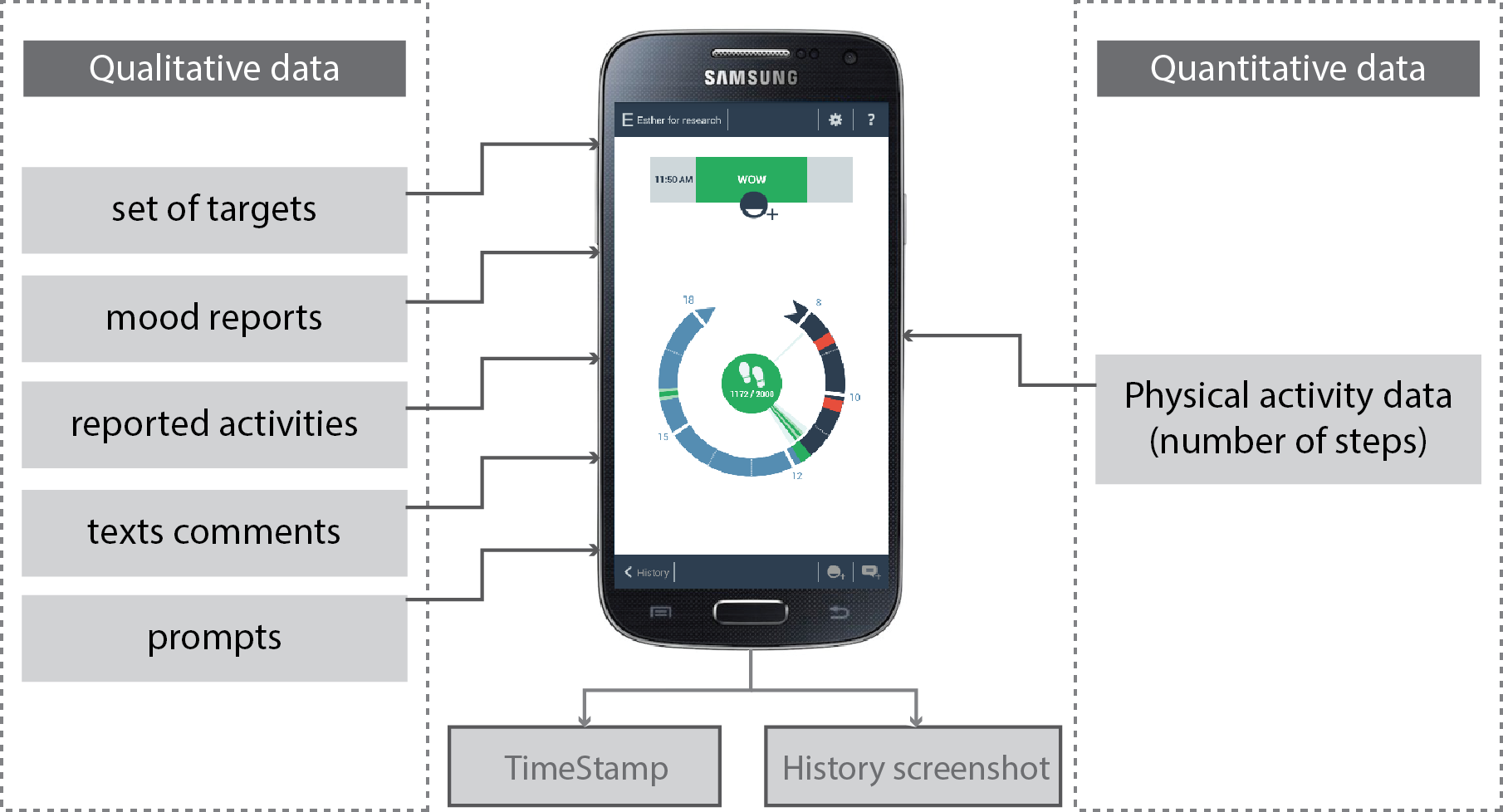
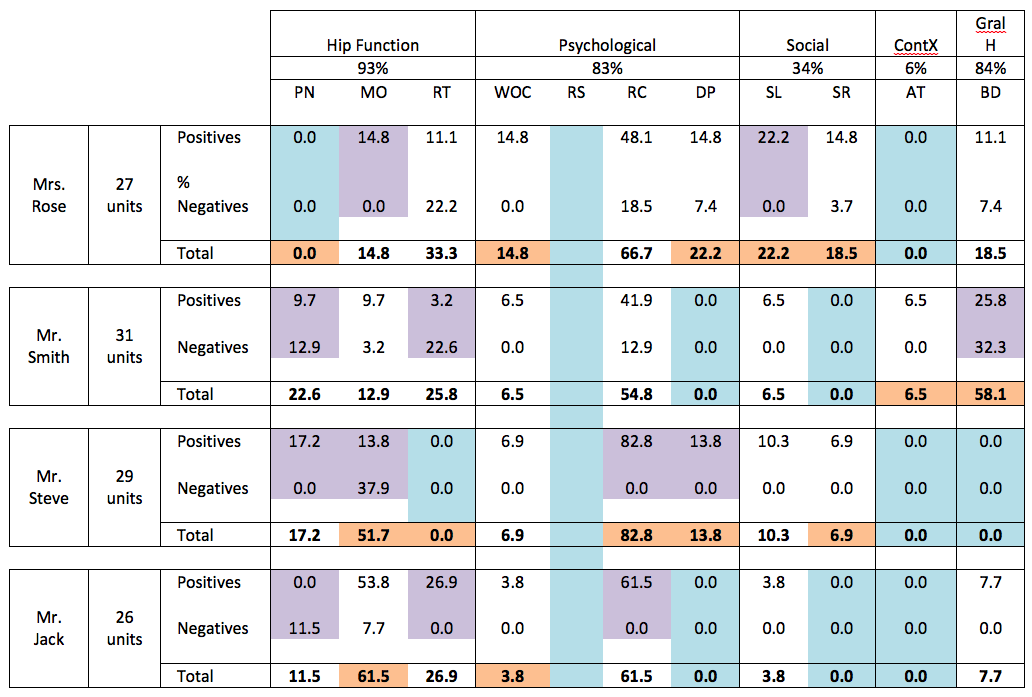
The implementation of field studies with the three prototypes resulted in a considerable amount of qualitative and quantitative raw data. Based on Grounded Theory framework GT (Glaser and Strauss , 1967), different units of coding analysis were developed to describe the sensitivity longitudinal and granularity of the self-reported data. In addition to response rate, average lengths of the reports, and time between prompts and responses, sensed data from sensors were quantified and then linked to the self-reporting prompts. Following, some samples of different data analysis visualization:




Conclusions
ESTHER 1.0 revealed the value of the ESM platform in serving as a reflective mechanism to support patients. The facilitation of self-reporting techniques was found as a means to achieve a sense of self-reflection and empowerment among users. ESTHER 1.2 underlined the potential of self-reporting as a mechanism to increase awareness about users’ health process through describing feelings and events. Interestingly, participants experienced the system as becoming a companion in their process, identifying a clear user experience benefit, beyond clinical outcome. Preliminary results of the ESTHER 1.3 study showed that mCRs can serve as a supportive and valuable element for motivating non-physically active participants. mCRs supported them in having a better performance in achieving physical activity targets overtime. While the more physically active participants also showed an improvement in achieving targets, they assigned more value to the assistive elements of the application.
